Explore our featured cases/drug class reviews to enhance your learning
Do you have a Case that you think other students or colleagues would be interested in learning from?
Submit your Case to info@digitaldentalnotes.com
Oral Pathology Cases



These Cases are presented by
our
Board Certified Oral Pathologist
Dr Ashley Clark
Do you have a question for Dr. Clark? Please email your question to info@digitaldentalnotes.com
Oral Pathology Case 1 (Photo credit Dr. Marcos Garcia)
Question
What is the MOST likely diagnosis for this lesion?
- Fibroma
- Central giant cell granuloma
- Squamous cell carcinoma
- Peripheral ossifying fibroma

Answer & Explanation
Answer: D. Peripheral ossifying fibroma
This month’s case features a bump on the gum. The main differential diagnosis for these lesions include pyogenic granuloma, peripheral giant cell granuloma, and peripheral ossifying fibroma.
The main entities in the differential diagnosis are all reactive lesions rather than true neoplasms. They represent a growth on the gingiva occurring in response to something such as calculus build up. In pathology, the word ‘peripheral’ means ‘on the gingivae’ – therefore, the only place one can encounter a peripheral ossifying fibroma or peripheral giant cell granuloma is the gingiva. Though 75% of pyogenic granulomas occur on the gingivae, they can also occur anywhere in the oral cavity. Pyogenic granulomas are also known as “pregnancy tumors” as they occur with higher frequency in pregnant women, though men and non-pregnant women can also get pyogenic granulomas.
The best treatment for these lesions is surgical excision with submission for histologic evaluation. This is the treatment for a couple of reasons – first, the lesions will not go away without a biopsy. Second, we do need to rule out the rare cases of malignancy presenting as reactive bumps on the gum. Inform the patient that all three have about a 10-15% recurrence rate.
Board pearls :
1. The main differential diagnosis for bump on the gum is pyogenic
granuloma, peripheral ossifying fibroma, and peripheral giant cell
granuloma
2. The pyogenic granuloma is known as the pregnancy tumor; it is the only
one that can occur off the gingivae
3. Treatment is excisional biopsy with submission for histologic evaluation;
the recurrent rate is 10-15%
Oral Pathology Case 2 (Photo credit Dr. Ashley Clark)
Question
A 47-year-old woman presents with a white patch on her palate. It is removable with gauze. What is the MOST likely diagnosis?
- Leukoplakia
- Leukoedema
- Candidiasis
- Nicotine stomatitis

Answer & Explanation
Answer: C. Candidiasis
Candidaisis is by far the most common oral fungal infection in humans and is caused by Candida albicans. There are four main clinical patterns:
1. Pseudomembranous
2. Erythematous
• Median rhomboid glossitis (central papillary atrophy)
• Chronic multifocal
• Angular cheilitis
• Chronic atrophic (Denture stomatitis)
• Acute atrophic (Antibiotic sore mouth)
3. Chronic hyperplastic
4. Mucocutaneous
1. Pseudomembranous is the most easily recognizable and is often referred to as thrush. Removable white plaques are the hallmark of this infection.
2. Erythematous candidiasis is red rather than white
and cannot be wiped away.
o Median rhomboid glossitis appears in adults as a red area in the midline
posterior dorsal tongue and is directly anterior to the circumvallate
papillae.
o Chronic multifocal presents as multiple red areas in the oral cavity.
o Angular cheilitis occurs at the corners of the mouth where saliva can
pool. Edentulous adults with a decreased vertical dimension of occlusion
are at most risk. This form occasionally has a bacterial component as
well. Cheilocandidiasis can occur if a patient with angular cheilitis
licks their lips or places a balm on the angular cheilitis and spreads
the infection throughout the lips.
o Chronic atrophic candidiasis is striking redness under the denture-bearing
area; the denture will harbor most of the organism.
o Finally, acute atrophic candidiasis may occur after a course of broad-spectrum
antibiotics. It can cause loss of filiform papillae and a burning sensation.
Many of the symptoms in acute atrophic candidiasis are similar to those
noted in patients with xerostomia.
3. Chronic hyperplastic candidiasis is a white area that cannot be wiped away. Upon biopsy, numerous Candidal organisms are discovered. It typically occurs on the anterior buccal mucosa.
4. Mucocutaneous candidiasis presents as a severe form of oral candidiasis associated with immune dysfunction. The nails, skin, and other mucosal surfaces may also be involved. Associated systemic findings may include endocrine abnormalities or iron-deficiency anemia. Syndromic mucocutaneous candidiasis may also occur; these patients may be at an increased risk for malignancy.
Diagnosis can be made clinically. If histology is used, a PAS or GMS stain highlights the organisms. Treatment is with topical nystatin (a polyene agent) or clotrimazole (an imidazole agent). Systemic medications include fluconazole (a triazole). Ketoconazole is a systemic imidazole agent but should not be used for first round therapy for oral candidiasis as it requires an acidic environment for absorption and about 1 in 10,000 develop liver toxicity.
Oral Pathology Case 3 (Photo credit Dr. Marcos Garcia)
Question
What is the most likely diagnosis for this lesion?
- Mucocele
- Squamous papilloma
- Squamous cell carcinoma
- Peripheral ossifying fibroma

Answer & Explanation
Answer: B. Squamous papilloma
This month’s case features a squamous papilloma. These are very common benign lesions, occurring in 1 of 250 patients. Squamous papilloma’s are the most common epithelial tumor of the soft palate. They have a low virulence and infectivity rate, meaning they are not very contagious. Lesions tend to present as pedunculated, exophytic, white or mucosal-colored, wart-like growths and are typically about 0.5 cm in greatest diameter. These lesions are not considered sexually transmitted, nor do they have any association with HPV-driven oropharyngeal squamous cell carcinoma. Treatment is conservative surgical excision with an excellent prognosis.
Radiology Cases



These Cases are presented by
our
Board Certified Oral Radiologist
Dr Trishul Allareddy
Do you have a question for Dr. Allareddy? Please email your question to info@digitaldentalnotes.com
Radiology Case 1

A 40-year-old male complains of pain in the mandibular left first molar region. A pantomograph was made.
Radiographic findings: A radiolucent area associated with the apical regions of the mandibular left first molar. The entity has well-defined thin corticated borders and has a hydraulic appearance. The first molar has recurrent caries in close proximity to the pulp chamber.
Interpretation: Radicular cyst
Other Incidental findings: There is a dome-shaped radiopaque mass in the floor of the right maxillary sinus. The entity has the density of soft tissue; the appearance is consistent with a mucus retention phenomenon (pseudocyst). No treatment is necessary for this condition.
Radiology Case 2
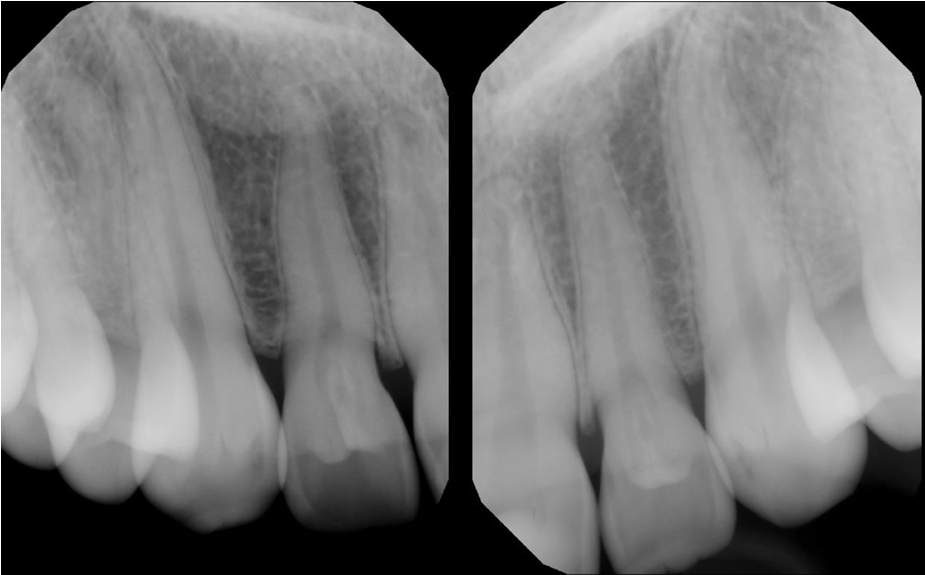
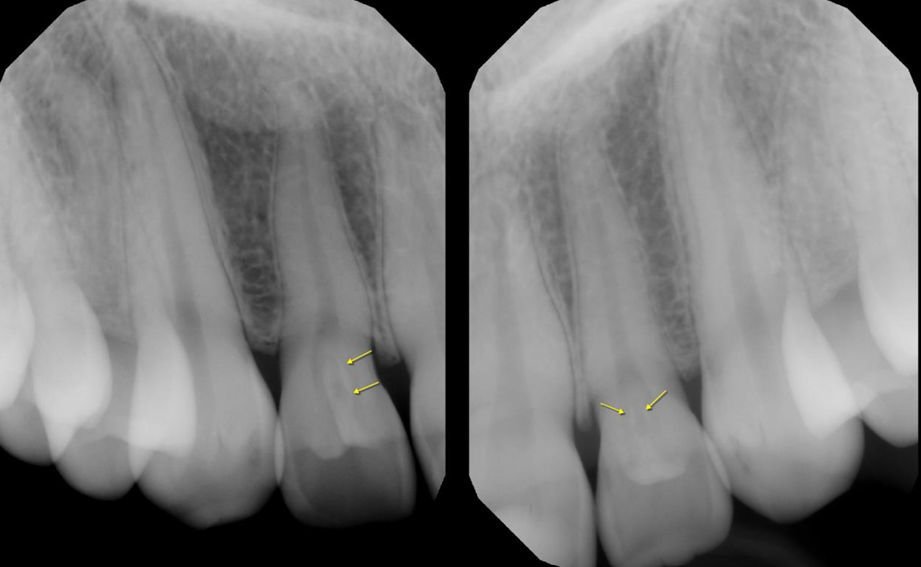
A 16-year-old female came in for a routine examination, upon clinical examination, periapicals of the maxillary anterior region were ordered.
Radiographic findings: Radiographs reveal well-defined radiolucent infoldings within the crown of the lateral incisors, outlined by a thin radiopaque enamel/dentin border. The invaginations extend almost up to the root.
Interpretation: Dens invaginatus in the maxillary lateral incisors
Treatment: In the absence of periapical inflammatory signs, prophylactic sealing is recommended.
Pharmacology Drug Class Reviews



The following Drug Class reviews are presented by
our
Board Certified Pharmacologist
Tom Viola, R. Ph., C.C.P.
Do you have a question for Tom? Please email your question to info@digitaldentalnotes.com
Pharmacology Drug Review 1 : SSRI’s
Pharmacology Drug Review 2 : Benzodiazepines
Would you like to see a particular lesion/topic covered?
Please submit your request to info@digitaldentalnotes.com